FREQUENTLY ASKED QUESTIONS
Amyloidosis is a rare group of diseases characterized by the abnormal buildup of a protein called amyloid in organs and tissues throughout the body. This protein can interfere with normal function and cause damage to affected areas, leading to potentially serious health complications.
Types of Amyloidosis
- AL Amyloidosis (Light Chain Amyloidosis)
- The most common form, caused by the overproduction of abnormal light chain proteins by plasma cells in the bone marrow.
- Affects organs such as the heart, kidneys, liver, and nerves.
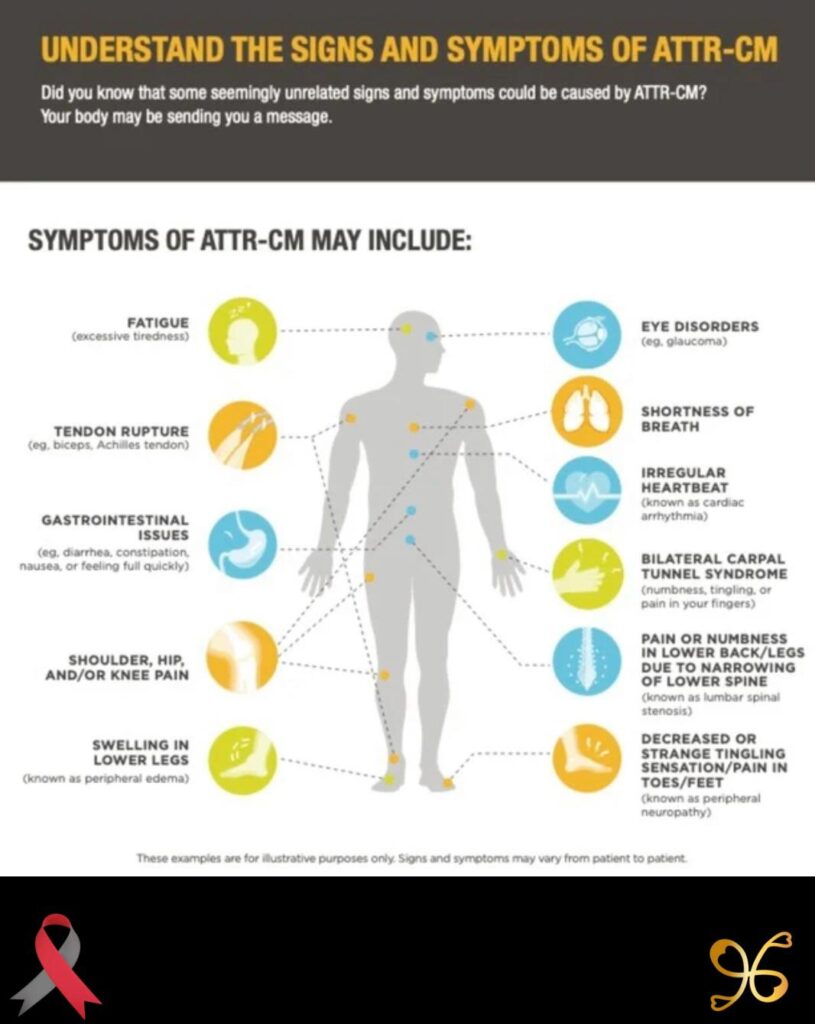
- ATTR Amyloidosis (Transthyretin Amyloidosis)
- Caused by mutations in the transthyretin (TTR) gene or by age-related changes to the protein.
- Subtypes:
- Hereditary ATTR Amyloidosis: A genetic condition affecting the nerves and heart.
- Wild-Type ATTR Amyloidosis: Typically affects older adults, primarily impacting the heart.
- AA Amyloidosis
- Results from chronic inflammatory or infectious diseases, such as rheumatoid arthritis or tuberculosis.
- Often affects the kidneys.
- Localized Amyloidosis
- Amyloid deposits occur in a single area of the body, such as the skin or bladder, rather than throughout the body.
- Other Rare Types
- Includes forms like Beta-2 Microglobulin Amyloidosis, often associated with dialysis.
Symptoms
Symptoms depend on the organs affected and may include:
- Fatigue or weakness.
- Shortness of breath.
- Swelling in the ankles or legs.
- Unintended weight loss.
- Tingling or numbness in the hands or feet.
- Enlarged tongue or difficulty swallowing (in some cases).
- Irregular heartbeat or heart failure (if the heart is affected).
- Kidney failure or protein in the urine.
Diagnosis
- Blood and Urine Tests: Detect abnormal proteins.
- Biopsy: A tissue sample confirms amyloid deposits.
- Imaging Tests: Evaluate organ damage (e.g., echocardiogram, MRI).
- Genetic Testing: Identifies hereditary forms of amyloidosis.
Treatment
Treatment focuses on managing symptoms, slowing disease progression, and addressing the underlying cause:
- Medications: Target amyloid deposits or reduce protein production (e.g., tafamidis for ATTR amyloidosis, chemotherapy for AL amyloidosis).
- Organ Transplants: For severe cases affecting organs like the heart or liver.
- Supportive Care: Treats complications such as heart failure or kidney issues.
Relevance to the Black Community
- Awareness and Access to Care: Like many rare diseases, amyloidosis may go underdiagnosed in underserved communities due to lack of awareness or healthcare access.
- Genetic Predispositions: Some hereditary forms, like ATTR amyloidosis, may disproportionately affect individuals of African descent.
Early detection and a multidisciplinary approach to treatment are essential to managing amyloidosis effectively. Collaboration with specialists and access to resources can improve outcomes and quality of life for those affected
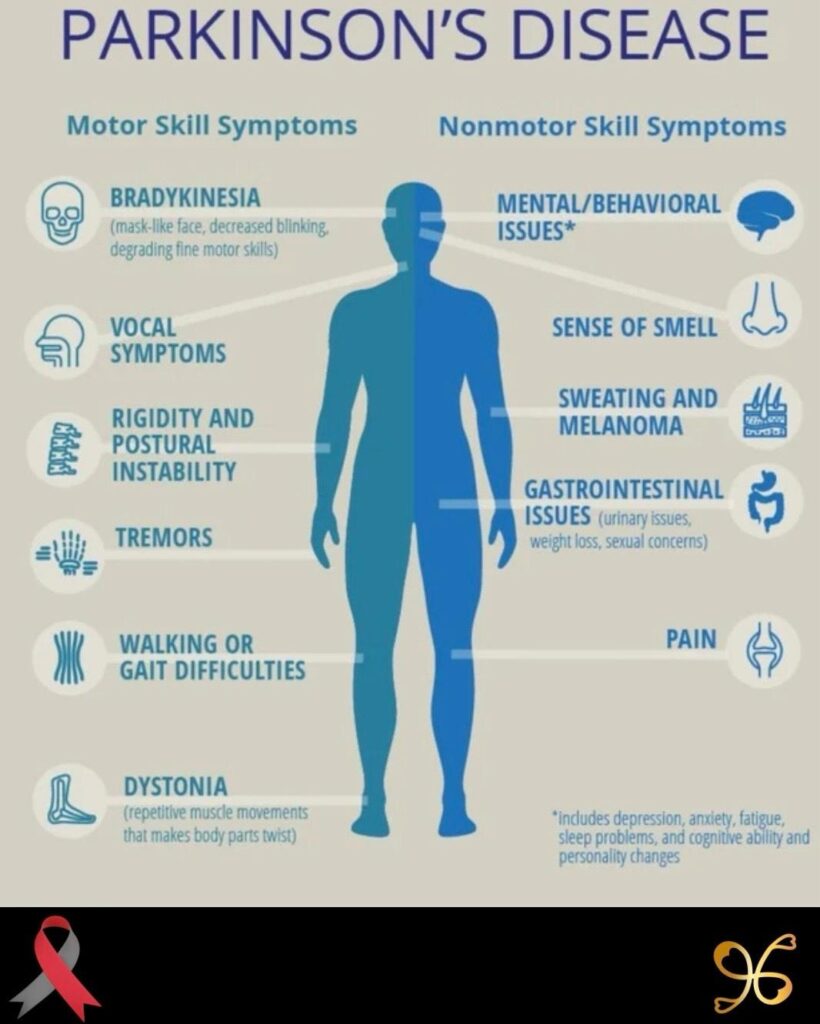
Parkinson’s Disease is a progressive neurological disorder that affects movement, coordination, and various non-motor functions. It results from the loss of dopamine-producing neurons in a region of the brain called the substantia nigra, leading to the characteristic symptoms of the disease.
Symptoms
Parkinson’s Disease has a wide range of motor and non-motor symptoms:
Motor Symptoms
- Tremors: Shaking, typically starting in the hands or fingers, even at rest.
- Bradykinesia: Slowness of movement, making simple tasks time-consuming.
- Rigidity: Stiff muscles that may cause pain or limit range of motion.
- Postural Instability: Problems with balance and coordination, leading to a higher risk of falls.
Non-Motor Symptoms
- Cognitive changes, including memory issues or difficulty concentrating.
- Depression and anxiety.
- Sleep disturbances, such as insomnia or REM sleep behavior disorder.
- Fatigue.
- Constipation and other gastrointestinal issues.
- Loss of sense of smell (anosmia).
Causes
The exact cause of Parkinson’s is unknown, but several factors contribute to its development:
- Genetics: Mutations in certain genes (e.g., LRRK2, PARK7) can increase risk, though hereditary cases are rare.
- Environmental Factors: Exposure to toxins such as pesticides or heavy metals.
- Age: Risk increases significantly with age, typically affecting people over 60.
- Gender: Men are slightly more likely to develop Parkinson’s than women.
Diagnosis
Parkinson’s is diagnosed clinically, as no definitive lab test exists:
- Neurological Exam: Focused on motor function and reflexes.
- Imaging Tests: MRI or PET scans rule out other conditions.
- Response to Medication: Improvement with dopamine-replacement therapy supports diagnosis.
Treatment
While there is no cure, treatment focuses on managing symptoms and improving quality of life:
- Medications:
- Levodopa: Converts to dopamine in the brain to alleviate motor symptoms.
- Dopamine Agonists: Mimic dopamine’s effects.
- MAO-B Inhibitors: Slow the breakdown of dopamine.
- Surgical Options:
- Deep Brain Stimulation (DBS): Implants electrodes in the brain to regulate abnormal activity.
- Lifestyle and Supportive Therapies:
- Physical, occupational, and speech therapy.
- Regular exercise to improve mobility and balance.
- Dietary adjustments to manage constipation and maintain energy levels.
- Mental Health Support:
- Counseling for anxiety or depression.
- Support groups for patients and families.
Parkinson’s in the Black Community
- Underdiagnosis and Delayed Treatment: Parkinson’s may be underrecognized in Black patients due to healthcare disparities or biases.
- Awareness and Access: Outreach and education are critical for improving early diagnosis and care in underserved communities.
- Research Gaps: Increased representation in clinical studies is needed to understand disease progression and outcomes in Black populations.
Living with Parkinson’s
Parkinson’s requires a multidisciplinary approach, involving neurologists, therapists, and caregivers. With proper management, many patients maintain independence and lead fulfilling lives for many years after diagnosis. Early intervention and a supportive network are key to improving quality of life.
Diagnosing Amyloidosis can be challenging because symptoms often resemble other conditions. There is usually not one single test that confirms amyloidosis. Instead, physicians use a combination of blood tests, urine tests, imaging studies, genetic testing, and tissue biopsies.
Key Tests Used to Confirm Amyloidosis
- Blood Tests
These help determine if abnormal proteins are present.
- Serum Free Light Chain Assay (FLC)
- Detects abnormal light chains produced by plasma cells.
- Very important for diagnosing AL (Light Chain) Amyloidosis.
- Serum Protein Electrophoresis (SPEP)
- Looks for abnormal proteins in the blood.
- Serum Immunofixation Electrophoresis (IFE)
- More sensitive than SPEP for detecting monoclonal proteins.
- Cardiac Biomarkers
- NT-proBNP
- BNP
- Troponin
- Help determine whether the heart is affected.
- Urine Tests
- 24-Hour Urine Collection
- Urine Protein Electrophoresis (UPEP)
- Urine Immunofixation
These tests look for abnormal proteins being excreted through the kidneys.
- Tissue Biopsy (Gold Standard)
A biopsy is generally required to definitively confirm amyloidosis.
Common biopsy sites include:
- Abdominal fat pad
- Bone marrow
- Kidney
- Heart
- Liver
- Nerve tissue
The tissue is stained with Congo Red stain.
When viewed under polarized light, amyloid deposits show the classic:
- Apple-green birefringence
This finding confirms amyloid deposition.
- Mass Spectrometry Typing
Once amyloid is found, doctors must determine the type.
Mass Spectrometry is considered the most accurate method for identifying:
- AL Amyloidosis
- ATTR Amyloidosis
- AA Amyloidosis
- Other rare forms
This is critical because treatment depends on the amyloid type.
- Cardiac Testing (If Heart Involvement Is Suspected)
Echocardiogram (ECHO)
Can show:
- Thickened heart walls
- Diastolic dysfunction
- Enlarged atria
- Preserved ejection fraction despite symptoms
Cardiac MRI
Often reveals:
- Characteristic amyloid infiltration patterns
- Late gadolinium enhancement
Nuclear Scan (PYP Scan)
One of the most important tests for ATTR Amyloidosis.
Common scans:
- Technetium-99m PYP Scan
- DPD Scan
- HMDP Scan
A strongly positive PYP scan combined with negative monoclonal protein testing can often diagnose ATTR cardiac amyloidosis without a heart biopsy.
- Genetic Testing
If ATTR Amyloidosis is suspected, genetic testing can determine whether it is:
- Hereditary ATTR (hATTR)
- Wild-Type ATTR
This is especially important in African American families because a genetic variant called Val122Ile (V122I) is more common among people of African ancestry.
Tests Your Cardiologist May Order Based on Your Recent Echo
You previously shared an echocardiogram showing:
- Moderately increased left ventricular wall thickness
- Mild left atrial enlargement
- Preserved EF (60-65%)
- Indeterminate diastolic function
These findings do not confirm amyloidosis, but they can be seen in amyloidosis and several other conditions, including:
- Long-standing hypertension
- Hypertensive heart disease
- Hypertrophic cardiomyopathy
- ATTR cardiac amyloidosis
Given those findings, you may want to ask your cardiologist about:
- Serum Free Light Chain Assay
- SPEP and Serum Immunofixation
- UPEP and Urine Immunofixation
- NT-proBNP and Troponin
- Cardiac MRI
- Technetium-99m PYP Scan
- Genetic testing for ATTR if indicated
Questions to Ask Your Cardiologist
- Could my increased wall thickness be due to amyloidosis?
- Have I had serum free light chain testing?
- Have SPEP and immunofixation studies been completed?
- Would a PYP scan be appropriate?
- Would a cardiac MRI provide additional information?
- Do my echocardiogram findings suggest ATTR amyloidosis?
- Should I undergo genetic testing for hereditary ATTR?
- Should I be evaluated at an amyloidosis specialty center?
Major Amyloidosis Centers in the U.S.
- Amyloidosis Research Consortium
- Mayo Clinic Amyloidosis Program
- Boston University Amyloidosis Center
- Cleveland Clinic Amyloidosis Center
Unlike amyloidosis, there is no single blood test, urine test, MRI, or scan that definitively confirms Parkinson’s disease in most living patients. Parkinson’s disease is primarily a clinical diagnosis, meaning a neurologist—preferably a movement disorder specialist—diagnoses it based on symptoms, examination findings, and response to treatment.
Core Diagnostic Evaluation
- Neurological Examination (Most Important)
A neurologist looks for the cardinal signs of Parkinson’s disease:
- Resting tremor (shaking when the body part is at rest)
- Bradykinesia (slowness of movement)
- Rigidity (muscle stiffness)
- Postural instability (balance problems, usually later in the disease)
To diagnose Parkinson’s disease, a person typically must have:
- Bradykinesia
- Plus either tremor or rigidity
- Medical History and Symptom Review
Doctors evaluate symptoms such as:
Motor Symptoms
- Hand tremor
- Slowed walking
- Smaller handwriting (micrographia)
- Reduced arm swing
- Stooped posture
- Balance issues
- Soft voice
Non-Motor Symptoms
These can appear years before diagnosis:
- Loss of smell
- Constipation
- Sleep disturbances (especially REM Sleep Behavior Disorder)
- Anxiety
- Depression
- Fatigue
- Cognitive changes
- DaTscan (Dopamine Transporter Scan)
A DaTscan is the imaging study most commonly used to support a Parkinson’s diagnosis.
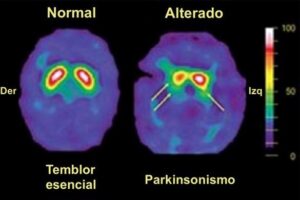
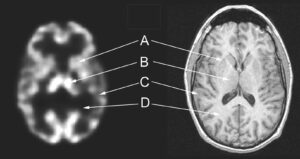
A DaTscan:
- Measures dopamine transporter activity in the brain.
- Can show whether dopamine-producing neurons are being lost.
- Helps distinguish Parkinsonian syndromes from conditions such as essential tremor.
Important:
- A DaTscan does not specifically prove Parkinson’s disease.
- It supports the diagnosis when clinical findings are unclear.
- Response to Levodopa
Many neurologists consider a significant improvement after taking:
- Carbidopa/Levodopa
to be strong evidence supporting Parkinson’s disease.
Patients with true Parkinson’s disease often show:
- Improved movement
- Less rigidity
- Better walking
- Reduced tremor
- MRI of the Brain
An MRI usually:
- Does not diagnose Parkinson’s disease.
- Helps rule out other conditions such as:
- Stroke
- Brain tumors
- Normal pressure hydrocephalus
- Multiple sclerosis
- Emerging Biomarker Testing
Researchers are developing tests that may improve diagnostic accuracy.
Examples include:
- Alpha-synuclein seed amplification assays
- Skin biopsies looking for abnormal alpha-synuclein deposits
- Cerebrospinal fluid (CSF) testing
These tests are becoming more available at specialized centers but are not yet universally used as standalone diagnostic tests.
Tests That Rule Out Other Conditions
Your physician may order:
- Thyroid function tests
- Vitamin B12 levels
- Complete blood count (CBC)
- Comprehensive metabolic panel (CMP)
These tests help exclude other causes of tremors, weakness, fatigue, or neurological symptoms.
Questions to Ask a Neurologist
- Do my symptoms meet the clinical criteria for Parkinson’s disease?
- Should I see a movement disorder specialist?
- Would a DaTscan be helpful in my case?
- Are there signs of another Parkinsonian disorder?
- Would a levodopa trial help clarify the diagnosis?
- What stage of Parkinson’s disease do you think I may have, if diagnosed?
- What therapies should begin immediately?
Major Parkinson’s Centers in the United States
- Parkinson’s Foundation
- Michael J. Fox Foundation for Parkinson’s Research
- Mayo Clinic
- Cleveland Clinic
- University of Florida Norman Fixel Institute for Neurological Diseases
For someone concerned about Parkinson’s disease, the most valuable next step is usually an evaluation by a movement disorder specialist, who has advanced training in diagnosing Parkinson’s and related neurological conditions. Early diagnosis can make a significant difference in symptom management, quality of life, and long-term planning